Laatst bewerkt: 10 juni 2025 (Wetenschappelijke bronnen toegevoegd bij de 2 dominante visies op DIS volgens de wetenschap)
The Keys methodology: a practice-based approach to DID
The integrated method I used to treat my own Dissociative Identity Disorder when the Dutch Mental Healthcare System failed me
APA referentie:
Van Stratum, L. C. (2025). Sleutelmethodiek: Een practice-based benadering bij DIS.
Geraadpleegd op (datum), van https://eendeelvanjezelf.nl/behandelstrategieen-bij-dis-lau-s-methode-/
Ethically relevant comments!
Self-treatment without guidance from a therapist or practitioner is not recommended. My method arose from a situation where I was stuck within the existing perspectives on dissociative identity disorder (DID) within the Dutch mental healthcare system. I found myself at a point where I saw no other option than to develop and implement my own treatmentmethod. However, during this process, I had a FACT team (without specialist knowledge of DID) with whom I had weekly supportive contact and could share everything. I developed, coordinated, and implemented the treatment myself, but I could share this with a FACT therapist (my psychiatrist), who monitored my suicidal behavior and ensured I was still acting responsibly.
Origin of my method
This process was born out of desperation, and I want to spare others with DID/complex trauma that very experience. That's why I'm sharing my personal approach. Because I believe it's important that treatment methods aren't information held behind a (pay)wall. The Key Method isn't (yet) an evidence-based treatment in the scientific sense, but is based on personal experience, existing treatment principles, and clinical reasoning.
Trauma treatment is a tailored practice! and not recommended otherwise
The treatment of complex trauma is a customized approach. Every person with DID/complex trauma is unique and has their own journey. What's described here is my personal interpretation and approach, which I hope will inspire and offer guidance. Important: I do NOT recommend this approach without a supportive social network or professional guidance. The loneliness and isolation this process can cause if you go it alone is of unspeakable depth, and I wouldn't wish this experience on anyone. Your relationships can also suffer, leading to further isolation.
Scientific substantiation? (June 10, 2025: 20% of 100% complete)
I'm well aware of the importance of scientific substantiation in mental healthcare. A more comprehensive version with APA sources and academic substantiation will be released in due course. But I also want to mention that the academic world has long considered my way of thinking "inappropriate" (see also: Schol is esspessially hard). This makes translating this personal work into academic language more demanding and emotionally draining for me. Nevertheless, I choose to do so, step by step. Because I believe that lived experience and science can and should reinforce each other.
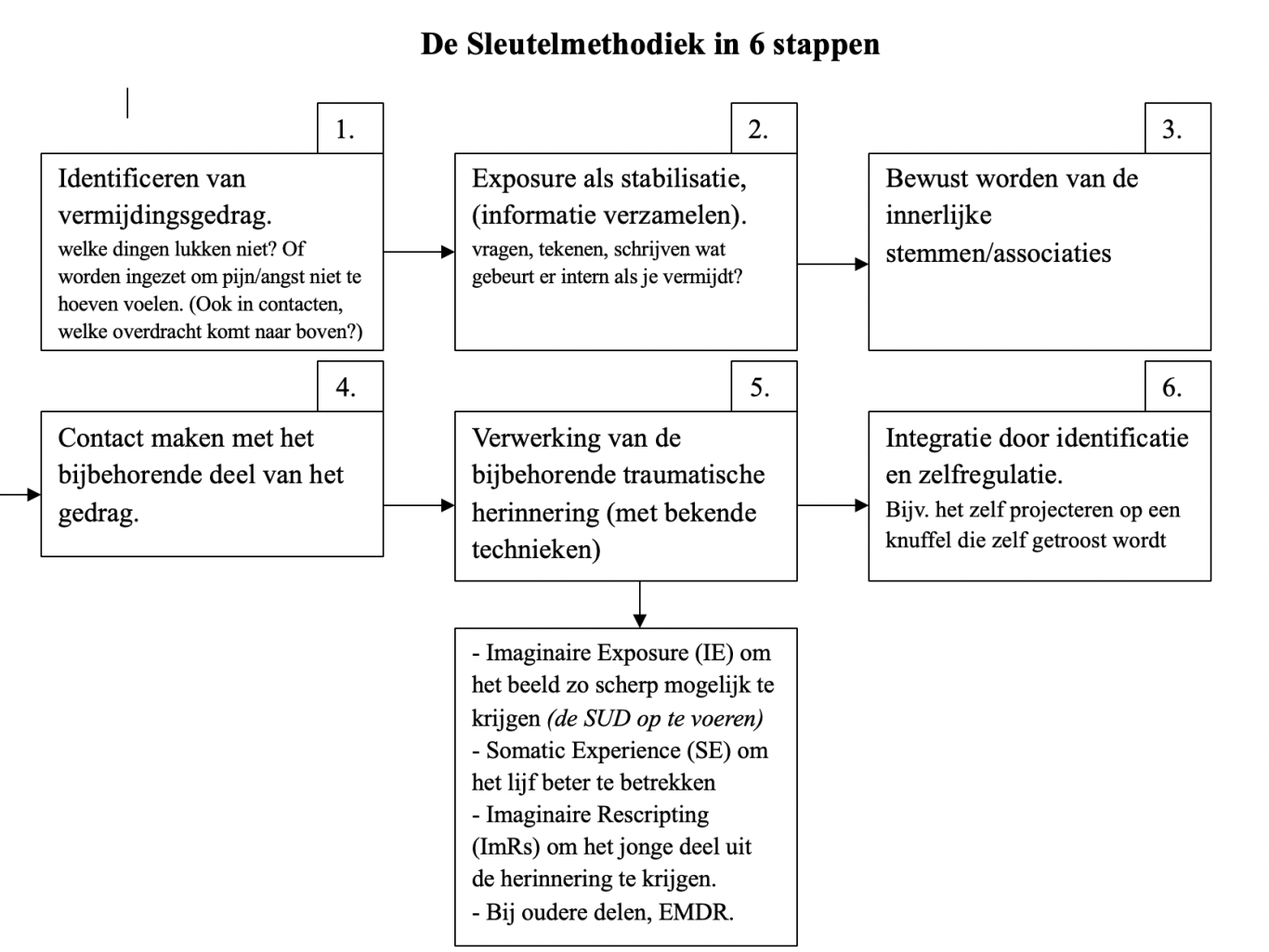
The button below contains a professional iterative treatment guideline that can be used as a practical framework for therapists and practitioners with prior knowledge of complex trauma. Beneath the schematic model, I authentically share my lived experience of my key method.
Preliminary: Contraindications
This method is not suitable for people who:
- are highly susceptible to psychosis
- have few reflective skills
- lack a strong social network
THEORY
An integrative vision: normalizing and recognizing
The core of this approach is exposure: shining a focused and mindful light on what is, by definition, excluded from consciousness. It is precisely this avoidance of awareness that is the primary reason why someone develops dissociative identity disorder (DID). The trauma is so deeply hidden that it remains invisible even to the conscious mind.
Within the Dutch mental healthcare system in 2025, two dominant perspectives on DID can be distinguished:
- Vision 1: Avoidance model
According to this view, parts in DID are seen purely as avoidance mechanism, in which the experienced amnesia is part of that avoidance. Studies by Huntjens et al. (2014) and Marsch et al. (2021) show that in DID so-called ‘apparent amnesia’ is subjectively perceived because tests show information transfer between identities (dissociative parts). This is in line with the view of Minnen & Huntjens that parts are avoidance mechanisms rather than physical memory barriers. Schema therapy for DID (STbijDID) recognizes and addresses parts as avoidance or mode mechanisms. In both the treatment protocol of Huntjens, Rijkeboer & Arntz (2019) and a recent case study by Bachrach et al. (2023), amnesia is seen as coping, in which schema therapy interventions are directly used to break through this avoidance.
- Vision 2: Functional trauma model/structural dissociation model (Phase model)
This model posits that in DID, the personality is divided into Apparently Normal Parts (ANPs) and Emotional Parts (EPs). ANPs carry daily functioning, while EPs are burdened with trauma and emotional charge. Trauma processing requires these parts to work together, and integration works best in a phased approach (stabilization → trauma processing → integration). (Van Der Hart & Steele, 2022). Parts carry the trauma and fulfill different functions, each with its own names and tasks. Trauma processing should be approached with caution in connection with true amnesia. This is the view of most TRTCs (Top Referent Trauma Centers) in the Netherlands, based on experience and conversations with several people with DID. This view is supported by recent research on the FSG program (Brand et al., 2025), an online intervention focused on psychoeducation and skills for people with complex dissociative disorders. In this RCT, the group with direct access to the program showed significant improvements in emotion regulation, PTSD symptoms, self-compassion, and adaptive capacity compared to the waitlist group. The results demonstrate that stabilization-focused interventions, provided they are structured, repeatable, and self-paced, are effective, especially for severely dissociative clients. Furthermore, the authors emphasize that their findings contradict a more aggressive approach that considers stabilization unnecessary. The results thus confirm the importance of a phased, stabilizing approach, as also employed in most TRTCs.
My vision (Keys Methodology) integrates elements of both the avoidance model and the structural dissociation model.
While the avoidance model emphasizes breaking through coping strategies and the structural-dissociation model emphasizes the importance of phased collaboration between parts, my experience shows that both perspectives can complement each other. A too-rapid approach aimed at unmasking avoidance can lead to retraumatization, while an overly prolonged focus on internal components sometimes perpetuates avoidance. By connecting both models through small-scale exposure and systematically gathering trauma-related key information, space is created for integration at one's own pace, while maintaining autonomy and direction. An integrative approach combining these two perspectives can provide the key to relatively rapid and lasting treatment for complex trauma.
Dissociative parts: protectors and signals of avoidance
Dissociative parts are split off "either from within the self or imposed by the environment" to protect the person from enduring the trauma. This means that a strong focus on the form of these parts (such as names, ages, hobbies, and internal relationships) can often align with the client's protective mechanism. It can prevent the client from having to address the underlying PTSD trauma. In other words, the elaborate naming and structuring of parts, keeping track of dozens of names, and creating an internal "community" that chats pleasantly about their separate activities can also be a form of safety behavior. This can be functional in the short term, but it simultaneously facilitates the processing of underlying trauma by avoiding it. As someone who has personally experienced both extremes -the suppression and denial of parts, as well as the over-explicit exaggeration of a DID image- I can confirm that both forms conceal the same painful trauma.
The Paradox: Addressing Trauma Without Overwhelming
A direct approach to the PTSD trauma is often not feasible in DID, due to the layered and complex nature of this disorder. After all, it is the dissociative parts that carry the trauma; you cannot ignore or deny this. Dismissing or denying these parts actually strengthens the protective mechanism underlying DID. This only perpetuates and sometimes even exacerbates the disorder. Although it may seem in the short term that the trauma has disappeared, what you are actually doing is pushing it down even deeper, similar to a ball being submerged underwater; at some point, it will forcefully shoot back to the surface. Although all the parts remain part of one person, postponing trauma processing only increases the distance from the underlying trauma. That distance grows with each postponement, making the step of facing the trauma increasingly difficult.
PRACTICE BASED TREATMENT
Key Principle: Exposure but make it very small
In my experience, exposure does not only begin with the trauma processing itself, but much earlier: with the (destructive) avoidance strategies that precede it.
Examples:
Do you find it difficult to eat? Then start by exposing yourself to that behavior, use a bit of CBT.
Write down, draw, or verbalize what resonates with you:
"What exactly is happening? What are you hearing inside yourself that's preventing you from eating? What's the worst that can happen? What are you afraid of?" Behind this fear often lies a still-unconscious reason, a key to an (still) unconscious memory.
Do you self-harm? Then examine what precedes this act.
Write down or visualize:
"What do you feel? What do you hear in your head just before you hurt yourself?"
This, too, contains a subconscious clue.
Do you avoid the bathroom, the shower, or going to the toilet?
Ask yourself:
"What's happening and what do you hear in your head as you walk there? What's the worst that could happen? What are you afraid of?"
This, too, points to a hidden fear, a clue.
Anything that makes your mind say, "I can't do this," could point to a deep-seated fear and deserves careful examination. This process is difficult, because every little piece of information surrounding the trauma can unconsciously trigger associations and fear. And that's often where the avoidance lies. However, gathering as much information as possible about these hidden feelings and fears holds the key to progress.
The Big Process: From all those Keys to underlying Core Trauma
With the information gathered, the "keys," you can take the next step: connecting with the corresponding dissociative part. This means inviting that part to talk about what happened and to feel the trauma, while you, as an inquisitive and caring adult, remain present. Ideally, a technique like ImRs (Imaginal Rescripting) can be applied here, in which the part is symbolically removed from the traumatic situation and you, as an adult, confront the perpetrator in the image. If the image isn't yet clear or deviates too much from how the trauma may have actually happened, Imaginal Exposure (IE), in which you gently relive the image without directly intervening, can help to make it more complete, so that Rescripting or, for example, EMDR is more effective afterward. In my own experience, it helped to connect with younger parts through symbols, such as a stuffed animal that represented the part I was comforting as if it were a younger version of myself. Such an external self-co-regulation tool promoted the integration of the memory as part of myself. If you can manage it at some point, I recommend drawing a snapshot from memory. With all the memories side by side, this will eventually create a kind of illustrated integrative timeline, as known from NET (Narrative Exposure Treatment).
⚠️ Be aware: Trauma processing is only effective if you can remain clear-headed enough to stand BESIDE the trauma. If you find yourself repeatedly sinking into flashbacks, this means you first need to gather more context around your avoidance and everything that's unconsciously stored.
A judgment-free unfolding process
This means that "recovered memories" are not something controversial, but a natural consequence of peeling back the layers, similar to what is known from EMDR for complex trauma (Poli et al., 2023; Sezis, 2023). The more you expose mild traumatic charge, the more space is created for processing deeper fears. This doesn't mean that you (or your client) deliberately exaggerate your story, or that external information "shapes" the trauma. This is about the dissociative amnesia that, through acknowledgment and recognition, increasingly gains space to integrate the full trauma, layer by layer. Treatment isn't about finding the truth, but about discovering what you're truly afraid of. Of course, influencing memory is a real risk. But the targeted collection of information about your own experiences, focusing on your emotional experience and bodily sensations, is actually illuminating. You are not a detective, and the therapist is not a judge. Treatment isn't about the exact details, like the color of your clothes in your memory. It's about recognizing what's so disruptive that you instinctively avoid it, often couched in thoughts like, "I'm not sure."
Explanation of why it worked for me (opinions may differ on this!):
Explanation through PTSD-model
In my view, dissociative identity disorder (DID) can be understood as a young, extreme form of post-traumatic stress disorder (PTSD). PTSD often develops when someone experiences an event that is too overwhelming to process all at once. Because the brain prefers to avoid this intense experience, the trauma remains unconscious, but the body and mind force processing through intrusions and reliving. The person then tries to avoid these painful memories as quickly as possible, thus perpetuating the mechanism until treatment breaks the cycle (Foa & Kozak).
DID as a juvinile PTSD
With DID, this overwhelming experience takes place in a very young child's brain, which is not yet capable of processing trauma. A child automatically seeks comfort, both internally and externally, but when that comfort is unavailable, consciousness splits. This dissociation protects the child from the overload and failure of its growing physical and psychological systems (DID is me, 2023). Avoiding the trauma therefore occurs at an unconscious, neurological level to enable survival. Because children are creative and yet lack a fully developed personality, various split-off parts emerge, but in essence, it is the same survival mechanism.
Recognize dissociative amenisia as a necessary protective mechanism, not avoidance.
Recognizing these dissociative components as real and functional is crucial for trauma processing. Reducing dissociative amnesia to a "delusional" coping strategy fails to appreciate the complexity and neurological foundation of dissociation. In conditioned DID, amnesia barriers can even result from administered substances such as drugs and electroshock, which exacerbate the memory loss. This explains the extreme memory loss that cannot simply be traced back to avoidance.
Preconditions and safety
With these insights, I managed to largely process the trauma of my DID -for which I was initially given a prognosis of eight years of treatment- at home within two years. Regarding my final memories and my broken trust in mental health services, I sought help from a psychologist again. ⚠️ Important: I do NOT recommend this approach without a supportive social network or professional guidance. The loneliness and isolation this process can cause are of unspeakable depth, and I do not wish this experience on anyone. Your relationships can also suffer as a result.
Attachment and transference: the key to healthy relationships
DID and recognizing safety
With dissociative identity disorder (DID), it's often difficult to reliably distinguish between who is safe and who isn't. This can lead you to react easily, based on past, childhood fears, to people who are actually safe in the present. This leads to projecting old fears onto others, which can be stressful for both you and the other person. An effective way to deal with this is to approach these projections, just like avoidance strategies, with an investigative and curious approach. Gather information about your feelings and thoughts surrounding these reactions.
Key figures as mirrors of one's own fear
For example, is there someone close to you to whom you feel extremely attached, or whom you fear will abandon you? And then you find yourself thinking the next moment that this person is deliberately ignoring you, making you angry or hurt? Or do you often experience that the people around you feel threatening, as if they want to harm you? I call these people your "key figures" because the emotions and reactions they evoke in you hold important keys to your recovery process. By examining and understanding these patterns, space is created for healing and the building of healthy, safe relationships.
Mapping your daily transference
Key figures can trigger strong transference reactions. These are feelings and behaviors that actually stem from past experiences, but are now playing out in relationships with people from the present.
Therefore, watchout for signs such as:
- Feelings of abandonment or fear of abandonment
- Unexplained anger or distrust
- An overwhelming need for approval or validation
Questions that can help identify transference
- What happens and what do I hear in my head and body when I see this person?
- What happens and what do I hear in my head and body when I don't see this person?
- Do I feel nauseous or dizzy at the thought of saying "something wrong" around this person?
- Do I feel very small around this person?
- Do I have a tendency to want to convince this person that I'm nice or good enough?
- What do I hear in my head then?
Indications of transference (trauma charged)
Anything that evokes anxious stress can point to transference, experiencing old feelings with people who are neutral or innocent in the present. This can manifest as, for example:
- An anxious hope of being seen.
- An anxious longing to be cared for.
- An anxious feeling that this person is going to hurt you (without any evidence).
- An anxious feeling that you want/need to share everything with this person.
- An anxious feeling of sexual arousal, perhaps even (without feeling sexually attracted to that person). etc.
Careful exploration as a door to recovery
Transference is essentially traumatic charge. Just as with avoidance, it's important to explore this process slowly and carefully—exposure, in other words. Often, underlying the transference is an unresolved pattern from the past that is being reactivated. By examining this pattern instead of immediately believing or following it, you open a door to recovery. These "key figures" can indirectly provide you with keys to processing and healing.
Finally, the key is balance
During your recovery process, try not to become dependent, even on your key figure. Let connection be a choice, not a necessity. However tempting dependency may feel, it ultimately undermines your growth. No emotionally mature person is completely dependent, regardless of what they've been through. And that's precisely what this process is about: growing up, in your own way.
Between dependency and hyper-independence
Complete dependence on a therapist may seem safe at times, but in the long run, it actually proves limiting. That's not an easy truth to face; I know from experience how devastating that dependence can feel and how real the underlying emptiness is. At the same time, it's important to recognize hyper-independence as an avoidance mechanism. It's avoiding connection, avoiding building trust, out of fear of being hurt again. Be gentler with yourself in this than I sometimes was. Because that, too, is a protective strategy. Understandable, but not always helpful. So the key lies in the middle. In balance. In learning to sense when you can accept support and when you can trust yourself. In learning to build healthy attachment without losing or giving yourself away.
But above all, and this has always been my deepest truth, something I even ended up writing on the walls of my bathroom to remind every part of me:
The key to your healing lays inside!
Even if you'd prefer to forget everything, that key remains within you. And only you can find it.
No one else. But you don't have to do it alone.
References:
Bachrach, N., Rijkeboer, M. M., Arntz, A., & Huntjens, R. J. C. (2023). Schema therapy for Dissociative Identity Disorder: a case report. Frontiers in Psychiatry, 14. https://doi.org/10.3389/fpsyt.2023.1151872
Van Der Hart, O., & Steele, K. (2022). The Theory of Trauma-related Structural Dissociation of the Personality. In Routledge eBooks (pp. 263–280). https://doi.org/10.4324/9781003057314-20
Brand, B. L., Schielke, H. J., Putnam, K., Pierorazio, N. A., Nester, M. S., Robertson, J., ... & Lanius, R. A. (2025). A randomized controlled trial assists individuals with complex trauma and dissociation in Finding Solid Ground. Psychological Trauma: Theory, Research, Practice, and Policy.
Huntjens, R. J. C., Wessel, I., Hermans, D., & Van Minnen, A. (2014). Autobiographical memory specificity in dissociative identity disorder. Journal Of Abnormal Psychology, 123(2), 419–428. https://doi.org/10.1037/a0036624
Huntjens, R. J. C., Rijkeboer, M. M., & Arntz, A. (2019). Schema therapy for Dissociative Identity Disorder (DID): further explanation about the rationale and study protocol. European Journal Of Psychotraumatology, 10(1). https://doi.org/10.1080/20008198.2019.1684629
Lebois, L. A., Ross, D. A., & Kaufman, M. L. (2021). “I Am Not I”: The Neuroscience of Dissociative Identity Disorder. Biological Psychiatry, 91(3), e11–e13. https://doi.org/10.1016/j.biopsych.2021.11.004
Marsh, R. J., Dorahy, M. J., Butler, C., Middleton, W., De Jong, P. J., Kemp, S., & Huntjens, R. (2021). Inter-identity amnesia for neutral episodic self-referential and autobiographical memory in Dissociative Identity Disorder: An assessment of recall and recognition. PLoS ONE, 16(2), e0245849. https://doi.org/10.1371/journal.pone.0245849
Poems about my own treatmentprocess (In Dutch)
Traumaverwerking thuis op de bank
Ik voel mij zo beroerd alles voelt wazig gaat er iets mis in mijn verstand?
Oke jongens let's fucking do this... we got this, niks aan de hand.
Ik zal naar je luisteren, wat probeer je mij te vertellen?
Ik weet niet of ik het wil geloven, het zal me beklemmen...
'Ik tiepe? zonder dat jij kijkt?'
Van mij mag alles, als je maar niet vermijdt.
Wat is dat vermijde?
Dat is de inhoud niet vertellen van waar je onder lijdt.
Het is het niet willen voelen van de onmenselijke strijd.
Maar ik zal je een geheimpje verklappen
Juist de verwerking blijven uitstellen is wat je zal vertrappen.
Het monster in de ogen kijken zal lucht geven
Ik zo ban, maa ik voor jou op sgrijfe.. ales trille en beve
het moes met mont,
zijn vies ding als een ijsje likke as ik goet verstont
Wat zie je in detail? Wat voel je? Wat moest je precies doen?
Kun je mij meenemen naar het verleden? Naar toen?
Alles begint te trillen Lau ik stik, ik ga straks over mijn nek, ik krijg geen lucht weet je zeker dat dit een goed idee is?
Zeker weten, de enige weg is erdoorheen, niks gaat mis.
Het gebeurd niet meer nu, ik ben bij je ik houd die man tegen laat de pijn niet los, maar doe je ogen eens open?
Ik huis zien. is hier nieman die mij kom sloope?
Nee het is voorbij.
Hier ben je alleen samen met mij.
Kijk eens, hier heb je je knuffel van een dinosaurus
Jaaaaa dinoooos. ik doe knufel geefe kus.
Zie je wel dat je het kan.
Ja ik nu hier ik nie meer ban
Je bent niet meer iemands bezit.
HOLY SHIT JONGENS WE HEBBEN ZELF TRAUMAVERWERKING GEDAAN, WE KUNNEN DIT!!!
LC, 2023
Teamwork
Zit je nou tegen jezelf te praten?
Wil je ons alsjeblieft laten?
Ik weet dat ik mij kan vertrouwen.
Dat we samen kunnen bouwen.
Maar dat we ook mogen rouwen.
Gevaar blijft daar. Het komt niet meer binnen wat zij ook mogen verzinnen.
Wat daders ook van ons willen.
Ik voel mij op momenten afhankelijk, maar nu ik zo van een afstandje kijk...
Ik hoef niet te leven naar jouw goedkeuring, als ik wil schelden zeg ik lekker tering. Ik hoef niet in jouw pas te lopen, ik hoef je mijn liefde niet te verkopen.
Ik besef mij dat ik het nooit zo heb kunnen zien, maar ik ben niet alleen, met DIS heb ik zelfs een heel team
- L, 12-05-2023
Interne communicatie
Zijn we elkaars beste maten? Nee. We kunnen elkaar écht haten.
Er is nijd er is strijd en altijd is er wel informatie kwijt. Of er heeft iemand spijt en er is sprake van veel lijd.
Ik zeg niet dat het makkelijk is, dat is wat ik bedoel.
Maar als de buitenwereld zorgt voor een onzeker en onbetrouwbaar gevoel. Vanuit alle pijn en paniek samen opzoek naar een doel.
Houdende het hoofd koel.
Zo communiceren wij via dit hoofd als natuurlijke paniek verzachter die de pijn verdoofd.
Want onszelf kunnen we niet wegjagen, nee we zullen dit samen moeten dragen.
Geen angst voor verlies juist omdat ik ipv voor de buitenwereld nu even voor interne communicatie kies.
- L, 12-05-2023
Samen strijden
Als de wereld uit elkaar valt, Als blijkt dat iets opnieuw ons leven vergalt.
Dan zijn wij niet alleen.
Dan praten wij samen, dan zijn wij 1 rotsvaste steen.
Als iedereen besluit weg te rennen.
Als men besluit ons niet meer te willen kennen.
Dan blijven wij met elkaar ook al is de buitenwereld dan heel naar.
We hebben onze verschillen.
De gedachte aan DIS doet mij nog altijd rillen.
Maar dan denk ik aan onze gesprekken onze angsten die hier mogen zijn.
Alles zonder consequenties die mogelijk leiden tot pijn.
Onze diepste verlangens per persoon ons geheim, als we maar blijven praten alleen dan zijn wij samen de lijm.
Vroeger klein en kwestbaar, vandaag: onverslaanbaar.
De daders hebben alles afgenomen van het kleine kind wat ze konden ze brachten aan de diepste fysieke, emotionele en seksuele wonden.
Maar door van zelf naar elkaar te splitsen blijven we ongeschonden.
We blijven met elkaar verbonden.
Want wij zijn samen de veiligheid die zij niet bieden konden.
-L, 12-05-2023
Suggestie
Ik ga je een geheim vertellen
Maar je mag het echt niemand uitspellen
Ik denk dat ik lieg over alles wat ik heb gezegd
Dat ik woorden in je mond heb gelegd.
…
Mag ik jou ook iets vragen?
Kan jij jouw verleden eigenlijk wel verdragen?
Want wat jij zegt klinkt als een vraag op een quiz.
En ik denk dat ik het antwoord weet.
Jij hebt namelijk een stoornis genaamd DIS.
- L 2022
Amnesie
Je doet mij zeer, en niet 1 keer maar steeds weer.
Dan weer spullen kwijt en vervolgens zorg je dat mijn studie eronder lijdt.
Dit kind liegt! Als verwijt. In mijn jeugd al zo vaak.
Ik doe niet alsof, al lijkt dat wel raak.
Taakjes verloren, zelfs nadat ik het had gezworen.
Ik ben echt eerlijk.. ik kan het niet meer weten.
Het feit is, Ik ben niet alleen vandaag,
Maar de helft van mijn leven vergeten.
- L 2022
Ontkenning
Ik moet iets bekennen, ik kan niet stoppen met ontkennen.
Dat wat zij mij hebben aangedaan, verdwijnt en kent geen bestaan.
Focus je toch op het heden.
Pas dan leef je een keer tevreden .
Maar ik leef gespleten, meer dan 1
En toch is het gelukt dat ik verdween.
Wie was ik dan
Wie zal ik zijn.
En wil ik dat wel weten als ik vervolgens verdrink in pijn?
Of zij wel echt zijn is mijn angst
Of ik niet lieg maakt mij misschien wel het bangst.
Dus wil ik weten wie ik ben…
Maar niet als ik daarmee het verleden erken.
- L- 2022