TPOY-2025-21-07-PSY
Between surrender and autonomy: A delicate balance in the treatment of complex dissociation and long-term traumatization
As a start I want to share this Dutch poem I wrote:
Brief aan alle hulpverleners
Ik wil je meegeven.
Wees in je vak bedreven.
Het kan veel zijn, soms ben je omgeven.
Maar blijf altijd gezonde professionele kaders nastreven.
Je bent een mens en je warmte moet je niet opgeven.
Als je twijfelt moet je dat bij je supervisor aangeven.
En ga bij jezelf altijd na, ben ik wel open en eerlijk in m’n werk gebleven?
En ik snap het, moeilijke dingen zitten vaak verweven.
Het gaat om precaire zaken het is regelmatig zelfs onbeschreven.
Maar aan sommige dingen mág jij gewoonweg niet toegeven.
Je hebt zoveel invloed… ik ben niet overdreven
Als ik zeg:
In jouw handen ligt een mensenleven.
LC, Juni 2024
Introduction
People with complex dissociation and prolonged trauma often find themselves in a long-term, dependent relationship with their therapists. The severity of the process makes trust in the other person feel essential, but this trust is often repeatedly betrayed, particularly due to a lack of knowledge and skills in the field of complex dissociation (Cronin et al., 2014; Myrick et al., 2015). This cycle of hope and disillusionment leaves deep scars (Papa et al., 2024) and calls for a reassessment of how we, as professionals, approach the treatment relationship in complex trauma.
Vulnerability to dependency
Treating complex trauma requires a long and intensive process. Many clients feel as if their recovery is entirely dependent on the therapist's knowledge, availability, and stability (Steele et al., 2001). This entails risks that, in my opinion, are often not explicitly discussed enough in practice:
Disadvantages of surrendering to the practitioner:
- The client finds themselves in an extremely vulnerable position, where their autonomy can be compromised.
- The process hinges on the therapist's expertise, which often leads to disappointment in practice.
- Outside of face-to-face contact, the process sometimes feels "on hold," as if it stalls without external guidance.
- A therapist's absence or change can have a retraumatizing effect, particularly on attachment trauma.
As I put it in a previous poem:
“In jouw handen ligt een mensenleven.”
Which translates to: "In your hands lies a human life."
This sentence encapsulates the immense impact that therapists can have. Many clients feel intensely dependent, while the therapist's capacity to cope is sometimes overestimated, and the client's autonomy remains underemphasized. As someone who has felt trapped in this dependent position, I know how undermining and damaging it can be to the recovery process when this cycle repeats itself over and over again.
Self-treatment out of necessity
For some people -myself included- the dependency on the skills of the therapist itself eventually became a threat. After years of inadequate treatment, the need arose to take charge of their own recovery process. A choice that fosters autonomy, but is far from ideal and often stems from necessity, not desire.
Disadvantages of self-treatment in complex dissociation and long-term traumatization:
- A balanced mirror is missing, allowing transference to focus on people outside the treatment context, risking relational damage.
- There is complete reliance on one's own frame of reference, leading to inevitable biases about one's own functioning.
- The feeling of loneliness increases significantly, accompanied by the thought: "This isn't how it should be..."
- Shame and self-reproach arise: "Is it my fault that I can't find suitable treatment?"
- Trust in healthcare, and sometimes in people in general, is deeply damaged.
The therapeutic alliance as education
What's desirable -and in my view, an underemphasized ideal- is a therapeutic alliance that helps the client continue independently, even if the therapist is absent (temporarily or permanently). Not by maintaining distance, but by transferring the knowledge. Good treatment, like training, focuses on transferring knowledge and skills. The therapist isn't a final destination, but a teacher who provides the tools and insights that ultimately enable the client to move forward independently.
In clinicalpractice, the opposite often happens in treatment of trauma:
The practitioner remains the expert and the client the recipient, which might increases the risk of renewed dependency and insufficient development of self-management.
Towards a new balance: relational autonomy
The challenge, therefore, lies in finding a balance: offering sufficient closeness and safety, without reducing the client to dependency. This requires conscious reflection on the following questions:
"Am I, as a therapist, actively transferring knowledge and tools?"
"Am I encouraging self-management, or am I unconsciously perpetuating the dynamic of dependency?"
"Would my client, if I was temporary unable to work, be able to independently (temporarily) build on what we have built together?"
Conclusion
In the treatment of complex trauma, the relational field is a risk area. Autonomy and trust are under pressure, and precisely for this reason, it is essential that therapists are aware of their role in this dynamic.
Not to shy away from responsibility, but to make it purposeful and transferable. Because only then can we build sustainable, supportive treatment. Not as an exclusive path, but as a shared journey with two experts: one expert in experience, and one expert in transferable knowledge.
Differences in the course of trauma processing in complex dissociation and long-term traumatization
Therapist-dependent, client without therapist & therapist + client themselves. (These are Simplifications based on my own experience & hypotheses. Not very ethical to research on a large scale 😉)
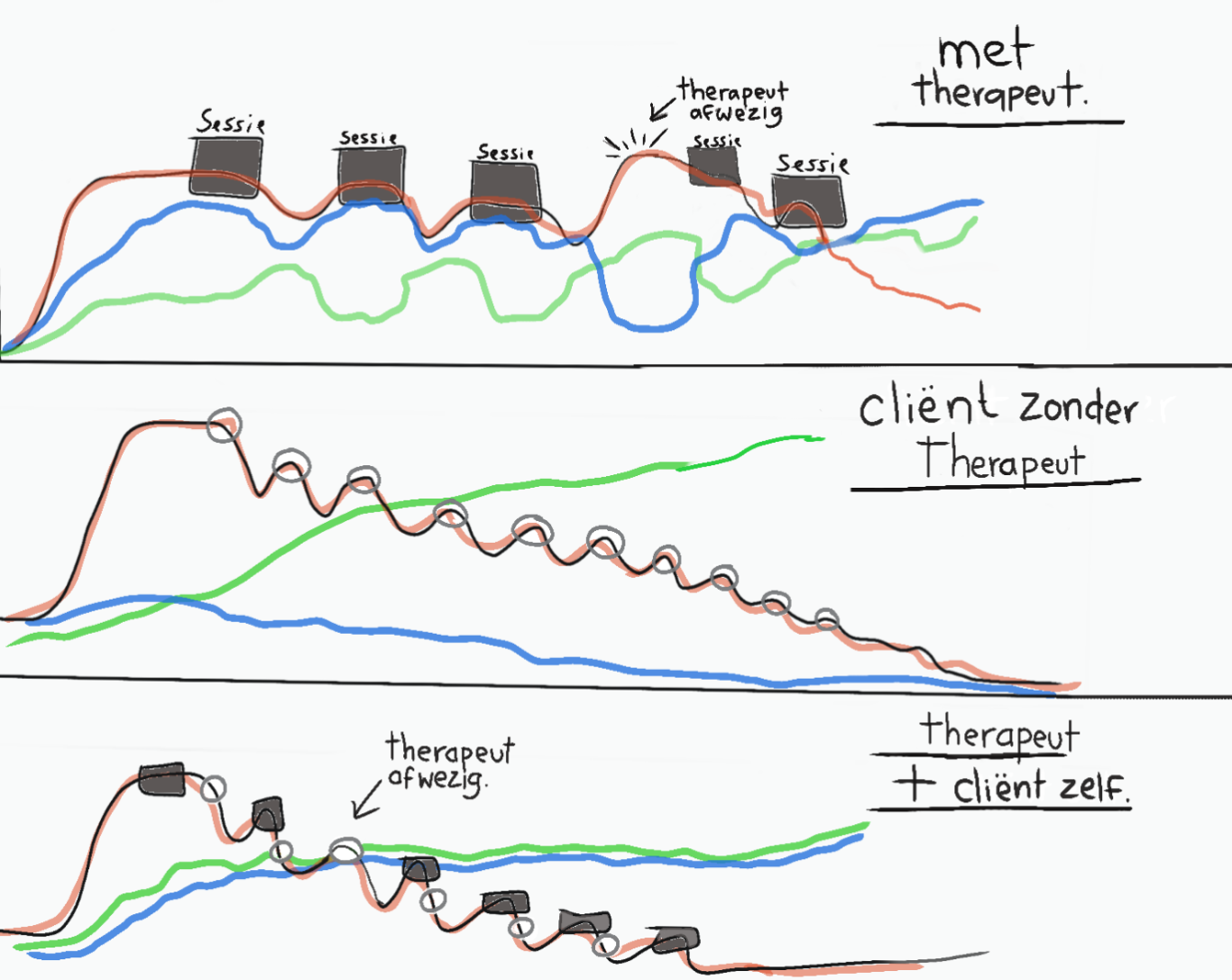
Note:
Red line: The SUD/traumarelated stress
Green line: The degree of self-direction / self-efficacy
Blue line: Trust (in other people)
Square: Session with therapist
Circle: Client does the session themselves
Explanation: (all simplifications, treatment processes depend on countless internal and external factors and can never be captured by a single factor):
1. Therapist-dependent (with therapist)
In the treatment of complex dissociation and long-term trauma, the relationship between client and therapist plays a significant role in the course of treatment. Experience shows that trauma-related tension (red line) fluctuates, as it were, with the therapist's availability. Consequently, a peak in tension is expected when the therapist is unavailable. If the therapist can be present congruently, trust (blue line) is expected to increase. When the therapist is unavailable, this can damage trust and put pressure on the entire process. The degree of self-control (green line) is expected to depend on the perceived trust in the therapist.
2. Client who treats himself without a therapist
The client who feels compelled to self-treat is likely to have become deeply disillusioned by the therapist's dynamic dependency. The moment the client initiates trauma processing techniques, their trauma-related tension (red line) will rapidly decrease at a pace appropriate to their processing speed. This significantly increases their sense of self-reliance and self-control (green line) during the process. However, self-treating trauma-related tension is perceived as highly unfair. And trust in others (blue line) continues to decline as the treatment progresses.
3. Autonomy-promoting therapist who transfers treatment techniques.
For the autonomy-promoting therapist who not only uses trauma processing techniques themselves but also provides them to the client and encourages them to use them themselves, the expectation is that trauma-related tension (red line) will decrease with minimal peaks. The client who is encouraged to use trauma processing techniques outside of treatment sessions is expected to experience a significant increase in perceived self-reliance and sense of self-control (green line), without this process compromising their trust in the therapist and others (blue line). These increases are expected to progress simultaneously, and the client is less likely to decompensate in the therapist's absence, as the therapist has the tools to manage the treatment themselves.
References in APA
Cronin, E., Brand, B. L., & Mattanah, J. F. (2014). The impact of the therapeutic alliance on treatment outcome in patients with dissociative disorders. European Journal Of Psychotraumatology, 5(1). https://doi.org/10.3402/ejpt.v5.22676
Myrick, A. C., Chasson, G. S., Lanius, R. A., Leventhal, B., & Brand, B. L. (2014). Treatment of Complex Dissociative Disorders: A Comparison of Interventions Reported by Community Therapists versus Those Recommended by Experts. Journal Of Trauma & Dissociation, 16(1), 51–67. https://doi.org/10.1080/15299732.2014.949020
Papa, C., Pugliese, E., Perdighe, C., Fimiani, R., & Mancini, F. (2024). ”I Am Longing and Afraid to Depend on You”: A Case Report on Breakdowns of Therapeutic Alliance and Interpersonal Cycles in Complex Trauma. Brain Sciences, 14(12), 1207. https://doi.org/10.3390/brainsci14121207
Steele, K., Van Der Hart, O., & Nijenhuis, E. R. S. (2001). Dependency in the Treatment of Complex Posttraumatic Stress Disorder and Dissociative Disorders. Journal Of Trauma & Dissociation, 2(4), 79–116. https://doi.org/10.1300/j229v02n04_05
APA-verwijzing:
Van Stratum, L. C. (2025). Tussen overgave en autonomie: de kwetsbare balans in behandeling van complexe dissociatie en langdurige traumatisering op (datum), van https://eendeelvanjezelf.nl/behandelstrategieen-bij-dis-lau-s-methode-/overgave-of-autonomie-